Alex Schadenberg
Executive Director – Euthanasia Prevention Coalition

On March 21, I reported that there were 4235 “Medical Aid in Dying” euthanasia deaths in 2018, an increase of 50% over 2017, representing approximately 1.5% of all deaths. The data for my report was obtained from a presentation by Jocelyn Downie, an academic euthanasia activist, for the March 15th Royal Society of Canada luncheon in Ottawa.
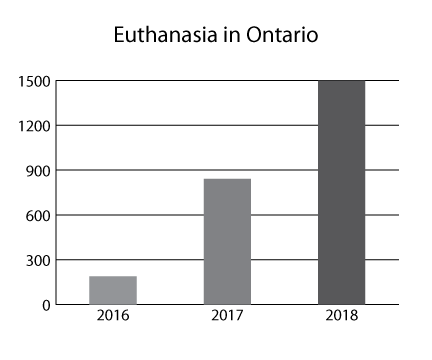
I have also reported the provincial data from Ontario and Alberta. The 2018 Ontario data indicated a 78% increase in euthanasia deaths while the 2018 Alberta data indicated a 50% increase. Further to that, last week I published an another article concerning the number of euthanasia deaths in Ontario and Alberta in 2019 (Link to the article).

On April 25, Health Canada released the Fourth Interim Report on Medical Assistance in Dying which stated that there were 2614 assisted deaths between January 1 – October 31, 2018. The report indicated that the data was incomplete for Quebec and the three Territories. The report incorrectly stated that assisted deaths represented 1.12% of all deaths in Canada. (Link to the report).
Using Statistics Canada’s available data for deaths per month in 2017 and projecting a 2% average annual increase in overall deaths (based on data trends from 2013 to 2017), we estimate that for the first 10 months of 2018, MAID has accounted for approximately 1.12% of the estimated total deaths in Canada during this reporting period.The data source they refer to is at: (Link).It gives a total of 276,689 deaths for all of Canada for 2017. Deducting the deaths for November 2017 (23,133) and December 2017 (25,141) gives a total of 228,415 for the 10 months Jan-Oct 2017. Applying the 2% increase the report suggests gives a presumed 232,983 deaths for all of Canada for the 10 months Jan-Oct 2018.
Health Canada does not appear overly concerned about the quality of the Medical Aid in Dying report. Basing percentages on an estimated, two percent increase in deaths is unacceptable. The data concerning the number of 2018 deaths in Canada does exist. Egan continues:
The report gives a total of 2,614 deaths by euthanasia for the same period Jan-Oct 2018 for Canada excluding Quebec. (And the NWT, Yukon and Nunavut for which there is also no data for 2017 deaths in the Statistics Canada death by months report.)The report appears to have divided 2,614 into 232,983 to get 1.12%. However the correct calculation should use as its denominator the presumed number of deaths for Jan-Oct 2018 for Canada excluding Quebec.There were 53,612 deaths in Quebec from Jan-Oct 2017. Subtracting these from the total for Canada of 228,415 for the 10 months Jan-Oct 2017 gives 174,803. Applying a 2% increase gives 178,299 presumed deaths in Canada other than Quebec from Jan-Oct 2018.Dividing 2614 into 178,299 gives a percentage of deaths by euthanasia of all deaths in Canada excluding Quebec of 1.47%.This more closely matches the data reported by Jocelyn Downie. She reports 4235 deaths by euthanasia for all of Canada (including Quebec) in 2018. The presumed number of deaths in all Canada in 2018 using the expected increase of 2% from 2017 data would be 282,222. 4235/282,222 = 1.5%.
Euthanasia deaths as a percentage of all deaths varies by province with British Columbia (2.37% of all deaths) nearly three times as deadly as Saskatchewan (0.84% of all deaths).
Other provincial rates are: Quebec 1.54% [Jan-Mar 2018]; Ontario 1.39%; Manitoba 1.25%; Alberta 1.18% and the Atlantic provinces (Newfoundland & Labrador, Prince Edward Island, Nova Scotia, New Brunswick) 0.98%.
One fact the fourth interim report did get right is what is really involved in what the Canadians euphemistically call MAID – medical assistance in dying:MAID is “an exception to the criminal laws that prohibit the intentional termination of a person’s life.”
MAID includes both euthanasia and assisted suicide. As of October 2018 there have only been six cases of assisted suicide under the Canadian law compared to 6743 cases of euthanasia.
This preference for euthanasia over assisted suicide has implications for Victoria (Australia) where both assisted suicide and euthanasia will be legal from 19 June 2019. While euthanasia is only permitted when a person is unable to physically self-administer or to digest the prescribed lethal substance this only requires one doctor to submit a form [Regulation 8 (b)] to the Secretary for Health making this assertion.